How Fasting Can Starve Cancer Cells, While Leaving Normal Cells Unharmed
People use the "curing cancer" as a metaphor for a giant achievement. There is no question that literally curing cancer would indeed be a giant achievement. Cancer is not only the second biggest cause of death, it can often be agonizingly painful. Moreover, the common cancer treatments of radiation and chemotherapy are awful experiences that can themselves cause lasting damage even if the cancer itself is defeated. So I was fascinated to read Thomas Seyfried's argument for another way to attack cancer in his book Cancer as a Metabolic Disease: On the Origin, Management, and Prevention of Cancer.
Cancer as a Metabolic Disease is not a well-written book. But it has an important set of ideas that are more mainstream than Thomas Seyfried lets on:
A majority of cancer cells have damaged metabolisms, often because delicate structures in their mitochondria—the folds called cristae—are damaged.
Metabolically damaged cancer cells can't produce as many handy ATP energy packets from each molecule of glucose (blood sugar). They can still produce ATP from the initial splitting of of a glucose molecule into two molecules of called glycolysis, which does not use oxygen. But they are not good at producing ATP from combining oxygen with the products of glycolysis to produce additional ATP.
This means that metabolically damaged cancer cells need to take in more glucose than normal cells to produce a given amount of ATP energy packets. They are more glucose-hungry than normal cells. So it helps cancer cells if glucose is abundant.
As an alternative to splitting glucose, cancer cells with damaged metabolisms can make ATP by using the energy in glutamine--an amino acid human bodies can make from many other amino acids.
Two key messages are that anything that boosts glucose or glutamine availability leads to better-fed cancer cells:
Eating sugar or other easily-digested carbohydrates is a good way to boost glucose levels in the bloodstream. Indeed, this is exactly what the glycemic index for different foods is designed to measure.
Eating high-protein foods is a good way to make amino-acids that can be turned into glutamine highly abundant. (It would be great to have measurements of a "glutamine index" for the effect of different foods on glutamine availability, parallel to the glycemic index.)
I am intrigued by cancer cells' ability to burn glutamine for energy in conjunction with the evidence for an association between protein intake and cancer that T. Colin Campbell and Thomas M. Campbell emphasize in "The China Study: Revised and Expanded Edition: The Most Comprehensive Study of Nutrition Ever Conducted and the Startling Implications for Diet, Weight Loss, and Long-Term Health." I wrote about that in "Meat Is Amazingly Nutritious—But Is It Amazingly Nutritious for Cancer Cells, Too?" At the time I wrote that post, I thought complete protein might be helpful as a raw material for the growth of cancer cells, which still might be true; but in addition, any kind of protein is likely to increase the availability of glutamine for cancer cells to burn.
The third key message is that fasting—a period of time without eating (while still drinking water)—will be harder on cancer cells than normal cells:
Fasting lowers glucose levels in the bloodstream. Normal cells can get a lot more ATP energy packets out of scarce glucose.
Fasting is likely to reduce glutamine availability.
Normal cells can burn fat during fasting. Cancer cells have a really tough time metabolizing fat. (During fasting, stored fat is often broken down to produce ketone bodies that circulate in the bloodstream to provide energy.)
If you actually get diagnosed with cancer, the current status of medical knowledge and the rules of medical ethics will mean your doctor will recommend that you try fasting only in conjunction with the usual treatments: surgery, radiation and chemotherapy according to standard protocols. But if you periodically fast as a preventative measure, you may starve cancerous or precancerous cells before you ever get diagnosable cancer. Fasting is relatively easy when you are eating foods low on the insulin index in any case. (See Forget Calorie Counting; It's the Insulin Index, Stupid.) And fasting is one of the best ways to lose weight, with all of the benefits from losing weight in reducing the risk of other diseases besides cancer. (See "Stop Counting Calories; It's the Clock that Counts" and "Obesity Is Always and Everywhere an Insulin Phenomenon.")
When I googled Thomas Seyfried, I found Orac's Respectful Insolence blog post "More hype than science: Ketogenic diets for cancer." Orac has two main points:
Thomas Seyfried is premature in recommending that people with diagnosed cancer depend on fasting and dietary changes to fight their cancer instead of surgery, radiation and chemotherapy. Much research should be done before that.
The idea of attacking cancer cells by their metabolic Achilles heel is now a mainstream idea, as I previewed above.
Consider these quotations from Orac's post, which is billed as critical of Thomas Seyfried:
Dr. Seyfried is a professor of biology at Boston College, who’s pretty well published. He’s also working in a field that has gained new respectability over the last five to ten years, namely cancer metabolism, mainly thanks to a rediscovery of what Otto Warburg discovered over 80 years ago. What Warburg discovered was that many tumors rely on glycolysis for their energy even in environments with adequate oxygen for oxidative phosphorylation, which generates the bulk of the chemical energy used by cells. ...
If you do a Pubmed search on “targeting cancer metabolism,” which is what Dr. Seyfried is talking about, you’ll find over 22,000 articles, with over 3,000 in 2013 alone, with a sharply increasing curve since 2000 that only now appears to be leveling off. A search on “cancer metabolism” brings up 369,000 references, with 28,000 in 2013 alone. Cancer metabolism is an incredibly important topic in cancer research and has been for several years now, and finding means of targeting the common metabolic abnormalities exhibited by cancer cells is currently a hot area of research. From my perspective, Dr. Seyfried is exaggerating how hostile the cancer research community is towards metabolism as an important, possibly critical, driver of cancer, although, to be fair, one prominent cancer researcher, Robert Weinberg, has been very skeptical.
After pointing out that, given current knowledge, human subjects review boards would insist on trying metabolic therapies on top of the standard approaches of surgery, radiation and chemotherapy, Orac writes:
... you might as well do a proper phase I/II clinical trial, which is what is happening. For instance:
Calorie-restricted, Ketogenic Diet and Transient Fasting During Reirradiation for Patients With Recurrent Glioblastoma (ERGO2), a randomized clinical trial designed to evaluate whether a calorie-restricted, ketogenic diet and transient fasting can enhance the efficacy of reirradiation in patients with recurrent glioblastoma.
Pilot Study of a Metabolic Nutritional Therapy for the Management of Primary Brain Tumors (Ketones), a phase I pilot study in my neck of the woods (at least in my state) looking at the same sort of diet.
Ketogenic Diet as Adjunctive Treatment in Refractory/End-stage Glioblastoma Multiforme: a Pilot Study, a small pilot study designed to examine the effect of a ketogenic diet in refractory GBM being treated with Avastin.
Ketogenic Diet With Radiation and Chemotherapy for Newly Diagnosed Glioblastoma, a phase I/II trial designed to test whether a ketogenic diet enhances the efficacy of radiation and chemotherapy.
In other words, clinical data should be rolling in fairly soon, and that’s a good thing.
Along the way, Orac points out that "only approximately 60-90% of cancers demonstrate the Warburg effect." To me, 60-90% sounds like a large fraction! What is more, in his book, Thomas Seyfried has what seem to me plausible criticisms of the experimental procedures used to conclude that some types of cancers can effectively oxidize the products of glycolysis. The basic problem, according to Thomas, is that to the unwary experimenter, metabolizing glutamine can generate indicators that create the illusion that a cancer cell is producing ATP by the oxidation of the products of glycolysis.
Orac's link above on the phrase "60-90% of cancers demonstrate the Warburg effect" is to the Science article "Energy Deregulation: Licensing Tumors to Grow" by Ken Garber. The claim 60-90% of cancers demonstrate the Warburg effect itself is attributed by Ken Garber to cancer biologist Craig Thompson.
In his article, Ken gives this useful background on metabolism in cancer cells:
[Eyal] Gottlieb, a biologist at the Beatson Institute for Cancer Research in Glasgow, U.K., notes that tumor cells need an unusual amount of energy to survive and grow. "The overall metabolic demand on these cells is significantly higher than [on] most other tissues," he says.
Tumors often cope by ramping up an alternative energy production strategy. For most of their energy needs, normal cells rely on a process called respiration, which consumes oxygen and glucose to make energy-storing molecules of adenosine triphosphate (ATP). But cancer cells typically depend more on glycolysis, the anaerobic breakdown of glucose into ATP. This increased glycolysis, even in the presence of oxygen, is known as the Warburg effect, after German biochemist Otto Warburg, who first described the phenomenon 80 years ago. Warburg thought this "aerobic glycolysis" was a universal property of cancer, and even its main cause.
Otto Warburg won a Nobel Prize for his work on respiration, but his claim that messed-up metabolism was a central cause of cancer fell out of favor. In Cancer as a Metabolic Disease, Thomas Seyfried provides strongly-argued modern rehabilitation of Warburg's theory of the origin of cancer. Thomas argues in detail that the oxidation of the products of glycolysis in "respiration" is crucial for maintaining the genetic stability and polite behavior of a cell: if cellular respiration fails, a cell usually dies, but sometimes manages to survive and go wild.
A key part of Thomas Seyfried's rehabilitation of Otto Warburg's claim about cancer origins is modifying Otto Warburg's idea that cancer cells derive their energy from splitting glucose to the idea that cancer cells derive their energy from splitting glucose and metabolizing glutamine. The mid-20th century criticisms of Otto Warburg's idea focused on his hypothesis that cancer derived their energy almost entirely from splitting glucose alone. These criticisms that, in Ken Garber's word, "discredited" Otto Warburg's ideas about the origins of cancer have much less bite against Thomas Seyfried's version in which cancer cells get energy from glutamine as well as glucose. Accounting fully for glutamine metabolism by cancer cells might raise the estimated percentage from Craig Thompson's "60-90% of cancers demonstrate the Warburg effect."
Regardless of whether damaged metabolism is important in the origins of cancer or not, the much less controversial proposition that cancer cells often have damaged metabolism means that fasting can stress out cancer cells a lot more than it stresses out normal cells.
I first learned about Thomas Seyfried in Jason Fung's book The Obesity Code. (See Five Books That Have Changed My Life.) Jason retails Thomas's advice to do a 7 to 10 day fast once a year in order to try to kill any cancerous or precancerous cells one may be hosting. I did that toward the end of 2017 and plan to do it again this year. I am a lot more scared of cancer than I am of fasting.
If I were ever diagnosed with cancer, the first thing I would do would be to begin fasting immediately; my hope would be to slow down the progress of the cancer during the time it took to develop a more conventional treatment strategy for my cancer. I would also do my best to try to convince my cancer doctor to read Thomas Seyfried's book in the hope my cancer doctor might get some good ideas for improving the treatment strategy.
I hope research on metabolic approaches to cancer treatment and cancer prevention continues at a brisk pace. Those outside the usual cancer research guild may well be able to think of ways to help the progress of this research.
For annotated links to other posts on diet and health, see:
For example, here is what the first section looks like:
I. The Basics
Tom Bartlett: What’s So Dangerous About Jordan Peterson? →
The link above takes you to a well-written and fascinating article by Tom Bartlett in the Chronicle of Higher Education on the now extremely controversial Jordan Peterson. Thanks to John Davidson for pointing me to this article.
Tom Bartlett found many he interviewed about Jordan Peterson unwilling to comment about on the record. This makes me worry greatly about the spread of guilt by association. Individuals should be held to account for things they say personally, but people should have a lot of leeway to hang out with--and even to say nice things about--individuals who have said arguably bad things.
Update: This post has sparked a vigorous and enlightening discussion on my Facebook page for it.
The Partitioned Matrix Inversion Formula

Image created by Miles Spencer Kimball. I hereby give permission to use this image for anything whatsoever, as long as that use includes a link to this blog. For example, t-shirts with this picture (among other things) and supplysideliberal.com on them would be great! :)
Is Milk OK?

Update, October 30, 2018: Make sure to read “Exorcising the Devil in the Milk” and “'Is Milk Ok?' Revisited” as well. There I write: “A1 milk is definitely not OK; A2 milk may well be OK other than a general caution not to consume too much animal protein.” The arguments below are better evaluated after reading “Exorcising the Devil in the Milk.”
I love milk. I also love high-quality cheese. So I am very reluctant (and unlikely) to give up consuming dairy products. But it is important to listen to those who are negative about dairy products and consider their arguments. Above, I take my pretty picture of milk from an otherwise random anti-milk webpage entitled "Myths About Milk You Probably Thought Were True." It mostly tries to attack positive notions about milk.
T. Colin Campbell and Thomas M. Campbell attack milk and other dairy products more directly in their book The China Study:
Animal Protein: The Campbells (father and son) have three basic arguments against milk. The first is that milk, like meat, has a lot of animal protein. I discussed this concern about animal protein in "Meat Is Amazingly Nutritious—But Is It Amazingly Nutritious for Cancer Cells, Too?" There I suggest this rule of thumb for a limit on animal protein per day:
I am thinking of a target of around 7% of calories in animal protein on a typical day, without trying to count up the amount of plant protein. ... The footnote at the end of Colin's passage suggests that 2200 calories a day would be typical for someone weighing 70 kilograms. ... 7% of that is 1 calorie per pound per day. ... about 1/4 of a gram of animal protein per pound of body weight per day.
I found by trying it out that for generic animal foods, you can google "how many grams of protein does [animal food x] have" and get a ready answer (with the specification of a measure of weight nice but often optional). For less generic animal foods—for example mozzarella cheese of a particular brand—one can look on the package. To provide some idea of magnitudes, a large egg has about 6 grams of protein, a cup of milk has 7.7 grams of protein, while a quarter-pound hamburger patty has about 29 grams of protein.
Inhibition of the Body's Production of the Active Form of Vitamin D
The Campbells' second argument against milk and other dairy products are that they inhibit the production of the active form of Vitamin D by providing too much calcium as well as because of the acidic internal environment engendered by animal protein. There is some suggestive evidence that the active form of Vitamin D is helpful in combating autoimmune diseases:
There are experimental animal models of lupus, MS, rheumatoid arthritis, and inflammatory bowel disease (e.g., Crohn’s disease, ulcerative colitis), each of which is an autoimmune disease. Vitamin D, operating through a similar mechanism in each case, prevents the experimental development of each of these diseases. This becomes an even more intriguing story when we think about the effect of food on vitamin D.
The first step in the vitamin D process occurs when you go outside on a sunny day. When the sunshine hits your exposed skin, the skin produces vitamin D. The vitamin D then must be activated in the kidney in order to produce a form that helps repress the development of autoimmune diseases. ... Under experimental conditions, the activated vitamin D operates in two ways: it inhibits the development of certain T-cells and their production of active agents (called cytokines) that initiate the autoimmune response, and/or it encourages the production of other T-cells that oppose this effect. (An abbreviated schematic of this vitamin D network is shown in Appendix C.) This mechanism of action appears to be a strong commonality among all autoimmune diseases so far studied.
The active form of Vitamin D also has other important functions in the body, as a passage from page 171 claims:
... active or “supercharged” D produces many benefits throughout the body, including the prevention of cancer, autoimmune diseases, and diseases like osteoporosis. This all-important supercharged D is not something that you get from food or from a drug. A drug composed of isolated supercharged D would be far too powerful and far too dangerous for medical use. Your body uses a carefully composed series of controls and sensors to produce just the right amount of supercharged D for each task at exactly the right time. As it turns out, our diet can determine how much of this supercharged D is produced and how it works once it is produced. Animal protein that we consume has the tendency to block the production of supercharged D, leaving the body with low levels of this vitamin D in the blood. If these low levels persist, prostate cancer can result. Also, persistently high intakes of calcium create an environment where supercharged D declines, thus adding to the problem. So what food substance has both animal protein and large amounts of calcium? Milk and other dairy foods. This fits in perfectly with the evidence that links dairy consumption with prostate cancer. This information provides what we call biological plausibility and shows how the observational data fit together. To review the potential mechanisms:
Animal protein causes the body to produce more IGF-1, which in turn throws cell growth and removal out of whack, stimulating cancer development.
Animal protein suppresses the production of supercharged D.
Excessive calcium, as found in milk, also suppresses the production of supercharged D.
Supercharged D is responsible for creating a wide variety of health benefits in the body.
Persistently low levels of supercharged D create an inviting environment for different cancers, autoimmune diseases, osteoporosis, and other diseases.
Here, from page 385, is a discussion of how milk might inhibit the production of the active form of Vitamin D. The active or "supercharged" Vitamin D is called 1,25 D:
Several studies now show that if 1,25 D remains at consistently low levels, the risk of several diseases increases. So then the question is: What causes low levels of 1,25 D? Animal-protein-containing foods cause a significant decrease in 1,25 D. These proteins create an acidic environment in the blood that blocks the kidney enzyme from producing this very important metabolite. A second factor that influences this process is calcium. Calcium in our blood is crucial for optimum muscle and nerve functioning, and it must be maintained within a fairly narrow range. The 1,25 D keeps the blood levels of calcium operating within this narrow range by monitoring and regulating how much calcium is absorbed from food being digested in the intestine, how much calcium is excreted in the urine and feces, and how much is exchanged with bone, the big supply tank for the body’s calcium. For example, if there is too much calcium in the blood, 1,25 D becomes less active, less calcium is absorbed, and more calcium is excreted. It is a very sensitive balancing act in our bodies. As blood calcium goes up, 1,25 D goes down, and when blood calcium goes down, 1,25 D goes up. Here’s the kicker: if calcium consumption is unnecessarily high, it lowers the activity of the kidney enzyme and, as a consequence, the level of 1,25 D. In other words, routinely consuming high-calcium diets is not in our best interests. The blood levels of 1,25 D therefore are depressed both by consuming too much animal protein and too much calcium. Animal-based food, with its protein, depresses 1,25 D. Cow’s milk, however, is high both in protein and calcium.
They emphasize the high-frequency nature of this process on page 382:
When needed, some of the storage form of vitamin D in the liver is transported to the kidneys, where another enzyme converts it into a supercharged vitamin D metabolite, which is called 1,25 D. The rate at which the storage form of vitamin D is converted to the supercharged 1,25 D is a crucial reaction in this network. The 1,25 D metabolite does most of the important work of vitamin D in our bodies. This supercharged 1,25 D is about 1,000 times more active than the storage vitamin D. Supercharged 1,25 D only survives for six to eight hours once it is made. In contrast, our storage vitamin D survives for twenty days or more. This demonstrates an important principle typically found in networks like this: the far greater activity, the far shorter lifetime, and the far lower amounts of the 1,25 D end product provide a very responsive system wherein the 1,25 D can quickly adjust its activity minute by minute and microsecond by microsecond as long as there is sufficient storage vitamin D to draw from. Small changes, making a big difference, can occur quickly.
Although the availability of the storage form of Vitamin D may not be that powerful in increasing the production of the active form of Vitamin D, a large enough amount may help significantly. See "Carola Binder—Why You Should Get More Vitamin D: The Recommended Daily Allowance for Vitamin D Was Underestimated Due to Statistical Illiteracy."
Personally, the thing I find reassuring in relation to any suppression of the production of the active form of Vitamin D by milk, cheese or animal protein in general is that any substantial period of fasting is likely to provide a period of time in which "supercharged" Vitamin D production will be uninhibited. In other words, in relation to the production of the active form of Vitamin D, it is constant consumption of milk and dairy products, or other animal protein that would cause the biggest problem. If there are frequent breaks from milk, dairy and animal protein consumption--as fasting for, say, 18 hours naturally provides--then there should be substantial chunks of time when the active form of Vitamin D is produced freely.
The Danger of Diabetes Type 1 from when Infants Drink Cow's Milk, and Possible Autoimmune Problems for Adults:
On page 179, the Campbells claim that having infants drink cow's milk raises the probability of Type 1 diabetes:
In the case of Type 1 diabetes, the immune system attacks the pancreas cells responsible for producing insulin. This devastating, incurable disease mostly strikes children, creating a painful and difficult experience for young families. What most people don’t know, though, is that there is strong evidence that this disease is linked to diet and, more specifically, to dairy products. The ability of cow’s milk protein to initiate Type 1 diabetes is well documented. The possible initiation of this disease goes like this:
A baby is not nursed long enough and is fed cow’s milk protein, perhaps in an infant formula.
The milk reaches the small intestine, where it is digested down to its amino acid parts.
For some infants, cow’s milk is not fully digested, and small amino acid chains or fragments of the original protein remain in the intestine.
These incompletely digested protein fragments may be absorbed into the blood.
The immune system recognizes these fragments as foreign invaders and goes about destroying them.
Unfortunately, some of the fragments look exactly the same as the cells of the pancreas that are responsible for making insulin.
The immune system loses its ability to distinguish between the cow’s milk protein fragments and the pancreatic cells, and destroys them both, thereby eliminating the child’s ability to produce insulin.
The infant becomes a Type 1 diabetic, and remains so for the rest of his or her life. This process boils down to a truly remarkable statement: cow’s milk may cause one of the most devastating diseases that can befall a child. For obvious reasons, this is one of the most contentious issues in nutrition today.
They summarize this argument on page 182:
It seems to me that we now have impressive evidence showing that cow’s milk may be an important contributor to Type 1 diabetes. When the results of all these studies are combined (both genetically susceptible and not susceptible), we find that children weaned too early and fed cow’s milk have, on average, a 50–60% higher risk of Type 1 diabetes (1.5–1.6 times increased risk). The earlier information on diet and Type 1 diabetes was impressive enough to cause two significant developments. The American Academy of Pediatrics in 1994 “strongly encouraged” that infants in families where diabetes is more common not be fed cow’s milk supplements for their first two years of life. Second, many researchers have developed prospective studies—the kind that follow individuals into the future—to see if a careful monitoring of diet and lifestyle could explain the onset of Type 1 diabetes. Two of the better known of these studies have been under way in Finland, one starting in the late 1980s and the other in the mid-1990s. One has shown that cow’s milk consumption increases the risk of Type 1 diabetes five- to sixfold, while the second tells us that cow’s milk increases the development of at least another three to four antibodies in addition to those presented previously. In a separate study, antibodies to beta-casein, another cow’s milk protein, were significantly elevated in bottle-fed infants compared to breast-fed infants; children with Type 1 diabetes also had higher levels of these antibodies. In short, of the studies that have reported results, the findings strongly support the danger of cow’s milk, especially for genetically susceptible children.
I find this quite scary in relation to feeding infants cow's milk. It also makes me worry that milk and other dairy products could have autoimmune effects on some adults. I am intrigued by the idea that absorption through the walls of the intestine before complete digestion could heighten autoimmune dangers. It also occurs to me that along the lines of the Campbell's thinking, it would be the combination of the initial autoimmune reaction from milk proteins and insufficient "supercharged" Vitamin D production that creates the greatest danger of autoimmune problems for adults. Periods of fasting would take away one of the two contributions to the danger.
I find myself somewhat at sea trying to evaluate the seriousness of dangers from milk and other dairy products. I would be glad to hear readers' perspectives on milk.
Don't miss these other posts on diet and health and on fighting obesity:
Anthony Komaroff: The Microbiome and Risk for Obesity and Diabetes
Using the Glycemic Index as a Supplement to the Insulin Index
How Fasting Can Starve Cancer Cells, While Leaving Normal Cells Unharmed
Meat Is Amazingly Nutritious—But Is It Amazingly Nutritious for Cancer Cells, Too?
The Case Against the Case Against Sugar: Seth Yoder vs. Gary Taubes
Carola Binder: The Obesity Code and Economists as General Practitioners
Jason Fung: Dietary Fat is Innocent of the Charges Leveled Against It
Faye Flam: The Taboo on Dietary Fat is Grounded More in Puritanism than Science
Confirmation Bias in the Interpretation of New Evidence on Salt
Putting the Perspective from Jason Fung's "The Obesity Code" into Practice
'Forget Calorie Counting. It's the Insulin Index, Stupid' in a Few Tweets
Julia Belluz and Javier Zarracina: Why You'll Be Disappointed If You Are Exercising to Lose Weight, Explained with 60+ Studies (my retitling of the article this links to)
Analogies Between Economic Models and the Biology of Obesity
Debating 'Forget Calorie Counting; It's the Insulin Index, Stupid'
Also see the last section of "Five Books That Have Changed My Life" and the podcast "Miles Kimball Explains to Tracy Alloway and Joe Weisenthal Why Losing Weight Is Like Defeating Inflation." If you want to know how I got interested in diet and health and fighting obesity and a little more about my own experience with weight gain and weight loss, see my post "A Barycentric Autobiography."
John Locke: The Law of Nature Requires Maturity to Discern

In the course of arguing that parental power is only temporary, John Locke makes it clear how closely reason is connected to his idea of natural law. Human beings are subject to natural law precisely because they have reason. And not just some degree of reason, the level of reason people have at maturity, assuming they have normal intelligence. In addition to making these key point in section 58-62 of his 2d Treatise on Government: “Of Civil Government” (Chapter VI. Of Paternal Power), John Locke gives a nice example of how crucial reason is to taking on one's role in society: even a king, if too young to have mature rationality, is not allowed full freedom. John Locke also points out that below a certain age, we do not require children to jump through the same hoops for citizenship that we require of adults:
The power, then, that parents have over their children, arises from that duty which is incumbent on them, to take care of their offspring, during the imperfect state of childhood. To inform the mind, and govern the actions of their yet ignorant non-age, till reason shall take its place, and ease them of that trouble, is what the children want, and the parents are bound to; for God having given man an understanding to direct his actions, has allowed him a freedom of will, and liberty of acting, as properly belonging thereunto, within the bounds of that law he is under. But whilst he is in an estate, wherein he has not understanding of his own to direct his will, he is not to have any will of his own to follow: he that understands for him, must will for him too; he must prescribe to his will, and regulate his actions; but when he comes to the estate that made his father a free man, the son is a free man too.
This holds in all the laws a man is under, whether natural or civil. Is a man under the law of nature? What made him free of that law? what gave him a free disposing of his property, according to his own will, within the compass of that law? I answer, a state of maturity wherein he might be supposed capable to know that law, that so he might keep his actions within the bounds of it. When he has acquired that state, he is presumed to know how far that law is to be his guide, and how far he may make use of his freedom, and so comes to have it; till then, somebody else must guide him, who is presumed to know how far the law allows a liberty. If such a state of reason, such an age of discretion made him free, the same shall make his son free too. Is a man under the law of England? What made him free of that law? that is, to have the liberty to dispose of his actions and possessions according to his own will, within the permission of that law? A capacity of knowing that law; which is supposed by that law, at the age of one-and-twenty years, and in some cases sooner. If this made the father free, it shall make the son free too. Till then we see the law allows the son to have no will, but he is to be guided by the will of his father or guardian, who is to understand for him. And if the father die, and fail to substitute a deputy in his trust; if he hath not provided a tutor, to govern his son, during his minority, during his want of understanding, the law takes care to do it; some other must govern him, and be a will to him, till he hath attained to a state of freedom, and his understanding be fit to take the government of his will. But after that, the father and son are equally free as much as pupil and tutor after non-age; equally subjects of the same law together, without any dominion left in the father over the life, liberty, or estate of his son, whether they be only in the state and under the law of nature, or under the positive laws of an established government.
But if, through defects that may happen out of the ordinary course of nature, any one comes not to such a degree of reason, wherein he might be supposed capable of knowing the law, and so living within the rules of it, he is never capable of being a free man, he is never let loose to the disposure of his own will (because he knows no bounds to it, has not understanding, its proper guide) but is continued under the tuition and government of others, all the time his own understanding is incapable of that charge. And so lunatics and ideots are never set free from the government of their parents; “children, who are not as yet come unto those years whereat they may have; and innocents which are excluded by a natural defect from ever having; thirdly, madmen, which for the present cannot possibly have the use of right reason to guide themselves, have for their guide, the reason that guideth other men which are tutors over them, to seek and procure their good for them,” says Hooker, Eccl. Pol. lib. i. sect. 7. All which seems no more than that duty, which God and nature has laid on man, as well as other creatures, to preserve their offspring, till they can be able to shift for themselves, and will scarce amount to an instance or proof of parents’ regal authority.
Thus we are born free, as we are born rational; not that we have actually the exercise of either: age, that brings one, brings with it the other too. And thus we see how natural freedom and subjection to parents may consist together, and are both founded on the same principle. A child is free by his father’s title, by his father’s understanding, which is to govern him till he hath it of his own. The freedom of a man at years of discretion, and the subjection of a child to his parents whilst yet short of that age, are so consistent, and so distinguishable, that the most blinded contenders for monarchy, by right of fatherhood, cannot miss this difference; the most obstinate cannot but allow their consistency: for were their doctrine all true, were the right heir of Adam now known, and by that title settled a monarch in his throne, invested with all the absolute unlimited power Sir Robert Filmer talks of; if he should die as soon as his heir were born, must not the child, notwithstanding he were never so free, never so much sovereign, be in subjection to his mother and nurse, to tutors and governors, till age and education brought him reason and ability to govern himself and others? The necessities of his life, the health of his body, and the information of his mind, would require him to be directed by the will of others, and not his own; and yet will any one think, that this restraint and subjection were inconsistent with, or spoiled him of that liberty or sovereignty he had a right to, or gave away his empire to those who had the government of his non-age? This government over him only prepared him the better and sooner for it. If any body should ask me, when my son is of age to be free? I shall answer, just when his monarch is of age to govern. “But at what time,” says the judicious Hooker, Eccl. Pol. l. i. sect. 6. “a man may be said to have attained so far forth the use of reason, as sufficeth to make him capable of those laws whereby he is then bound to guide his actions: this is a great deal more easy for sense to discern, than for any one by skill and learning to determine.”
Commonwealths themselves take notice of, and allow, that there is a time when men are to begin to act like free men, and therefore till that time require not oaths of fealty, or allegiance, or other public owning of, or submission to the government of their countries.
Civil law applies to adults in a way it doesn't fully apply to children, or those with mental incapacity. The same is true of natural law. In many ways, John Locke expects a lot of people, in seeing what is OK to do and what is not OK to do. But it is a beguiling picture of people gradually becoming able to see and understand natural law as they get older.
For links to other John Locke posts, see these John Locke aggregator posts:
Lisa Marshall: How Bright Light Keeps Preschoolers Wired at Night →
I wish I had known this when my kids were little.
Greg Ip: A Decade After Bear’s Collapse, the Seeds of Instability Are Germinating Again

In trying to avoid financial crises, as in wars, generals tend to prepare for the last war. In Greg Ip's retrospective "A Decade After Bear’s Collapse, the Seeds of Instability Are Germinating Again," Greg amplifies a 2014 warning by Hyun Song Shin to that effect by pointing out the wide variety of ultimately falsified ideas that have driven financial excesses and their ensuing crises:
Crises surprise because they usually start with an assumption so sensible that everyone acts on it, planting the seeds of its own undoing: in 1982 that countries like Mexico don’t default; in 1997 that Asia’s fixed exchange rates wouldn’t break; in 2007 that housing prices never declined nationwide; and in 2011 that euro members wouldn’t default. James Bianco, who runs his own financial research firm in Chicago, speculates that the equivalent today might be, “We will never see higher inflation or higher growth.” If either in fact occurs, the low interest rates that have raised household stock and property wealth to an all-time high relative to disposable income won’t be sustainable.
Rather than hoping to predict the shock that triggers the next financial crisis, we need to make the system more shock resistant. Bear's collapse provides a clue to how. Here is Greg Ip's brief explanation of that collapse:
Bear ... arranged mortgages that financed the housing bubble while borrowing heavily with short-term IOUs. When those mortgages went bad, Bear’s creditors yanked their funds—a de facto run on the bank.
In short, any financial institution is rickety if the people who gave you the money can pull their money out on short notice. If most of the funds behind a financial institution were given in return for long-term bonds—or even better, in return for stock—that financial institution is much more resistant to failure.
In the case of ordinary mainstreet consumer banks, we solved the danger from people being able to pull out their funds on a moment's notice with a government guarantee of deposits. We could have a system with explicit government guarantees of private bets in many places in the financial system, or a continued commitment to bailouts in the future that come as a surprise to the electorate. But if we don't want explicit government guarantees or an implicit government bailout policy, what we need to do is to put a cap on the amount of borrowing financial institutions can do—and especially the amount of short-term borrowing. This is another way of saying we need an upper limit on the amount of leverage that financial institutions can have and a lower limit on the amount of capital—equity—that a bank is financed by.
Though they wouldn't put it in these terms, banks and other financial companies don't like leverage limits because leverage limits limit their ability to make big profits by relying on an implicit too-big-to-fail or a too-many-to-fail expected bailout subsidy from the government. On this, see "Martin Wolf: Why Bankers are Intellectually Naked."
In Larry Summers's keynote speech at the October 22-23, 2015 University of Michigan Financial Stability Conference, he added two important angles on effectively regulating the financial system. At the 22:25 minute mark in this video of his speech, he points out a big problem financial regulation shares with many other forms of regulation: how would someone come to know enough about finance to be an effective regulator unless they either believed finance was a force for good in the world or mainly cared about earning a lot of money? In either case, they are likely to be "cognitively coopted" by the financial industry. It is possible for someone to believe that finance is a force for good in the world but that particular financial practices are very dangerous to the economy (indeed I put myself in that category), but an enthusiasm for finance often veers over into thinking that existing practices are good.
Larry Summers offers as a partial solution locating important chunks of financial regulatory power in the Federal Reserve. The Fed is a good choice for financial regulator because it has an outsized share of the few people who understand finance without being cognitively coopted by the financial industry. Larry doesn't say that explicitly; I do. Explicitly, Larry links his recommendation of the Fed as financial regulator to the idea that the Fed is long-lasting, prestigious institution—which makes it easier for the Fed to stand up to the financial industry. Of course, the Federal Reserve already has substantial financial regulatory powers. Maybe it should have more.
At the 27 minute mark, Larry points out that capital equity requirements and leverage limits are often stated in terms of book values on the balance sheet. The trouble with book values is that they our far out of date by the time a crisis occurs. The market values of a firm's stocks and bonds provide a much better early-warning system than those book values! Firms need to be required to have enough stockholder equity in the good times so that even if their stock prices tank, they still have enough of a cushion of stockholder equity that they won't go bankrupt. At a minimum, when a firm's stock price goes down enough that it doesn't have enough of a capital cushion by market prices, it should be forbidden to dissipate its capital cushion by paying dividends or buying back its own stock.
We have seen enough financial crises in recent years that those in charge can no longer plead ignorance that anything could go wrong. A decision to have low effective capital requirements, or to base those capital requirements only on book value, is a decision to play bailout roulette. Those who act to lower capital requirements or who resist raising them should be held to account now and in the future. The next big financial crisis and any associated bailout will be their fault. On the other side, if there is no "next big financial crisis" it will be either because capital requirements have been dramatically raised or because of an extraordinary streak of luck.
Let me note in closing that the depth and length of the Great Recession and its aftermath required two big mistakes. First, the mistake of having capital requirement too low. This led to the initial fall of the dominoes. Second, an inadequate monetary policy response, as I discuss in "America's Big Monetary Policy Mistake: How Negative Interest Rates Could Have Stopped the Great Recession in Its Tracks." I lay out the theory behind this view in "On the Great Recession" and have been working hard on the details of how to do effective negative interest rate policy, as you can see in "How and Why to Eliminate the Zero Lower Bound: A Reader’s Guide."
Carola Binder—Why You Should Get More Vitamin D: The Recommended Daily Allowance for Vitamin D Was Underestimated Due to Statistical Illiteracy
Note: At the bottom of this post I have links to my other posts on diet and health.
Carola Binder, like me, is blogging about diet and health. In her post "D is for Devastating: A Statistical Error and the Vitamin D Saga" she discusses the important news that the recommended daily allowance for Vitamin D should be more than ten times as big as it is. The recommendation of researchers who know what they are doing is 7000 IU. For me, that means this: In addition my regular multivitamin, each day I need to take three of the tiny 2000 IU Vitamin D3 gel capsules I get from Costco.
In general, it is better to get vitamins from natural sources when possible. But the most important natural source of vitamin D is sunshine. Short of giving up our indoor jobs, most of us are doomed to spend a lot less time outdoors than our ancestors, and so might not get enough Vitamin D from sunshine alone.
One indicator of the importance of Vitamin D to human health how quickly evolution lightened the skin tones of groups that left Africa and moved further from the equator. There is a substantial list of diseases that are more common at higher latitudes where there is less sunshine. T. Colin Campbell, in The China Study (a book I featured in "Meat Is Amazingly Nutritious—But Is It Amazingly Nutritious for Cancer Cells, Too?") argues that milk-drinking in high northern latitudes (and to a lesser extent, milk-drinking in high southern latitudes) is the problem. But the raw facts make me worry about the consequences of even mild Vitamin D deficiency. (It also makes me glad I moved to Colorado.) On page 383, T. Colin Campbell writes:
So far, we can see how adequate sunshine exposure, by ensuring enough storage form of vitamin D, helps to prevent cells from becoming diseased. This suggests that certain diseases might be more common in areas of the world where there is less sunshine, in countries nearer the North and South Poles. Indeed there is such evidence. To be more specific: in the Northern Hemisphere, communities that are farther north tend to have more Type 1 diabetes, multiple sclerosis, rheumatoid arthritis, osteoporosis, breast cancer, prostate cancer, and colon cancer, in addition to other diseases.
Researchers have known for eighty years that multiple sclerosis, for example, is associated with increasing latitude. As you can see in Chart C.2, there is a huge difference in MS prevalence as one goes away from the equator, being over 100 times more prevalent in the far north than at the equator. Similarly, in Australia, there is less sunshine and more MS as one goes farther south (r = 91%). MS is about sevenfold more prevalent in southern (43°S) than in northern Australia (19°S).
So it is a lot safer to assume that getting the right amount of Vitamin D matters than to blithely go on thinking you are getting the right amount of Vitamin D.
Too much Vitamin D can also be bad. So you have to get it right. As I noted above, the Wikipedia article on Vitamin D does not yet reflect what Carola says below. With both the official recommended daily allowance and the Wikipedia article off track, it might not be easy for you to get the real scoop on Vitamin D elsewhere. (It would be great if someone took it upon themselves to reflect Carola's post in the Wikipedia article on Vitamin D.)
As Carola discusses, Finland has already reformed it Vitamin D guidelines and has seen a decline in diabetes. Finland's Vitamin D fortification reform should also provide a test of how much of the extra multiple sclerosis, rheumatoid arthritis, osteoporosis, breast cancer, prostate cancer and colon cancer in high latitudes is due to Vitamin D deficiency. As other countries reform their Vitamin D guidelines, there will be more data for testing to what extent adequate Vitamin D can ward off these other diseases.
Below is Carola's account of how the current recommended daily allowance for Vitamin D came to be set at 600 IU instead of the more appropriate level of 7000 IU. Thanks, Carola, for permission to repost it here!
Statistical errors in research are quite common in research, and not always detected. As economists are well aware, when an error with important policy implications is revealed, it may prompt a media frenzy. I was surprised to learn recently of a major statistical error with potentially huge public health implications, yet with seemingly sparse media coverage when it was revealed.
The error concerns the Recommended Dietary Allowance (RDA) of Vitamin D. A 2014 paper found a statistical error in a study used by the Institute of Medicine (IOM) to determine the RDA, resulting in a recommendation that was about an order of magnitude too low.
I am neither a public health expert nor medically trained, but (following Miles Kimball's lead) have developed an interest in public health, and especially nutrition, research, largely due to its parallels with macroeconomic research. What little press coverage I did find about this Vitamin D study omitted technical discussion of the statistical error--"We'll spare you the gritty mathematical details," said one article. But I wanted these details, and so might you, so I dove in to what turned out to be a fascinating story. You may want to share it with your econometrics students: Correct interpretation of confidence intervals can truly be a matter of life and death.
First, some background. The human body can make Vitamin D (unlike other vitamins) when exposed to sunlight. It can also be attained by nutritional sources and supplements. Upon activation by the liver and kidneys, it acts as a hormone that plays a role in calcium metabolism. Sufficient Vitamin D is critical for bone health and a plethora of other health outcomes (more on that later). Research on the health effects of Vitamin D typically looks at health outcomes associated with different serum 25-hydroxyvitamin D (25(OH)D) levels (a measure of concentration in the blood).
The IOM issues dietary recommendations, including RDAs, for the US and Canada. The RDA is supposed to designate the nutrient intake sufficient to meet the needs of 97.5% of healthy individuals. For Vitamin D, issuing this guideline requires first deciding what 26(OH)D level is desirable, then deciding how much supplemental Vitamin D should be taken so that most people have the desired 26(OH)D level. Based on associations between 26(OH)D levels and various health outcomes, the IOM aimed to recommend an RDA that would result in 25(OH)D levels of 50 nmol/L or more.
The IOM then had to determine how much supplemental Vitamin D to recommend based on this goal. They looked at 10 studies of the dose response relationship of vitamin D intake and 25(OH)D. Some of these studies examined 25(OH)D levels for multiple different doses, so in total there were 32 estimates (the green diamonds in Figure 1). They fitted a dose response relationship curve to these points, with 95% confidence interval. The IOM came up with an RDA for individuals 1 to 70 years of age of 600 IU per day. You can see the vertical line at 600 in Figure 1. It intersects the fitted dose response curve at 63 nmol/L and the lower bound of the 95% confidence interval at 56 nmol/L. Remember, this was the amount that was supposed to achieve 25(OH)D levels of at least 50 nmol/L in at least 97.5% of healthy individuals.

Figure 1. Source: Veugelers and Ekwaru (2014)
In October 2014, Paul J. Veugelers and John Paul Ekwaru explained in a paper in Nutrients that the IOM's interpretation of these confidence intervals was incorrect. They thought that 2.5% of individuals would have serum levels below the lower 95% confidence interval, but in this meta-analysis, the unit of observation was not the individual, but the study average. In the authors' words:
The correct interpretation of the lower prediction limit is that 97.5% of study averages are predicted to have values exceeding this limit. This is essentially different from the IOM’s conclusion that 97.5% of individuals will have values exceeding the lower prediction limit.
Veugelers and Ekwaru returned to the 10 studies, eight of which reported both average and standard deviation serum level for particular doses of Vitamin D. From these statistics, the authors could calculate the 2.5th percentile at each dose. Then they regressed these 2.5 percentile values (the 23 yellow dots in Figure 2) on vitamin D intake, coming up with the red dashed line in Figure 2. The green dashed lines are the confidence intervals from Figure 1, for the sake of comparison.
In the figure, you can see that at 600 IU per day, 97.5% of individuals will have serum levels above around 27 nmol/L, not 50 nmol/L. To get 97.5% of individuals with serum levels above 50 nmol/L, you would actually need a higher dose than any of the studies examined. Out-of-sample extrapolation led them to estimate that 8895 IU of vitamin D per day would actually be required. Veugelers and Ekwaru also pointed to two studies in which 10% or 15% of Canadian subjects had serum 25(OH)D levels of less than 50 nmol/L despite vitamin D supplementation at the RDA level. They wrote, "If the RDA had been adequate, these percentages should not have exceeded 2.5%. Herewith these studies show that the current public health target is not being met."
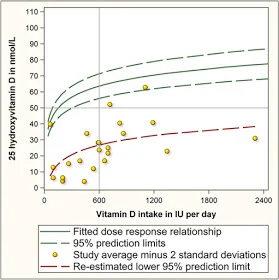
Figure 2. Source: Veugelers and Ekwaru (2014)
Veugelers and Ekwaru did caution that as 8895 IU of vitamin D per day "is far beyond the range of studied doses, caution is warranted when interpreting this estimate. Regardless, the very high estimate illustrates that the dose is well in excess of the current RDA of 600 IU per day and the tolerable upper intake of 4000 IU per day."
In March 2015, in the same journal, Robert Heaney, Cedric Garland, Carole Baggerly, Christine French, and Edward Gorham published a letter in the same journal that alleviated some of the concern about extrapolating beyond the available data. They presented entirely different data on individuals with daily vitamin D intakes from zero to over 10,000 IU. They came up with an estimate that was slightly lower than Veugelers and Ekwaru's, but confirming the finding that the IOM recommendation was around an order of magnitude too low, and wrote:
Thus, we confirm the findings of these investigators with regard to the published RDA for vitamin and we call for the IOM and all public health authorities concerned with transmitting accurate nutritional information to the public to designate, as the RDA, a value of approximately 7000 IU per day from all sources.
Like Veugelers and Ekwaru, Heaney et al. remarked upon the safety of such a high recommendation, though their take was more optimistic:
The total, all-source intake of 7000 IU/day is below the no observed adverse effect level (NOAEL) of both the IOM and the Endocrine Society, below the tolerable upper intake level (UL) of the Endocrine Society, and well within the safe range delineated by Hathcock et al., who had generated that range using the IOM’s method of hazard identification.
The hormonal role of vitamin D explains why the Endocrine Society also issues guidance about it. Remember, vitamin D is fat-soluble, so excess amounts are stored and can accumulate in body tissues-- hence the concern about safety at higher doses. Overall health benefits may increase with dose up to a point, and then start to decline. Initial guidelines on Vitamin D RDA were based on prevention of rickets. But as scientists have learned more about other health benefits, the cost-benefits calculus of vitamin D recommendations has shifted. This shift, however, was slow to be reflected inn health policy.
"Worldwide reports have highlighted a variety of vitamin D insufficiency and deficiency diseases. Despite many publications and scientific meetings reporting advances in vitamin D science, a disturbing realization is growing that the newer scientific and clinical knowledge is not being translated into better human health," wrote Andrew Norman in a 2008 issue of the American Journal of Clinical Nutrition. A 2007 article in the same journal, by Reinhold Vieth and many coauthors, describes the situation as a "frustrating and regrettable situation for nutrition researchers."
Vieth et al. summarize the many health benefits attributable to adequate vitamin D, and evidence that the tolerable upper limit is around ten times higher than officially-recommended intakes. But they point to an over-cautious and under-nuanced take by the public media that has kept public supplemental intake too low:
Evaluation of most relations of health and disease that involve vitamin D leads to the conclusion that a desirable 25(OH)D concentration is ≥75 nmol/L (30 ng/mL). If a concentration of 75 nmol/L is the goal to be achieved by consumption of vitamin D, then why is it so rare for members of the population to accomplish this? One reason is that almost every time the public media report that vitamin D nutrition status is too low, or that higher vitamin D intakes may improve measures of health, the advice that accompanies the report is outdated and thus misleading. Media reports to the public are typically accompanied by a paragraph that approximates the following: “Current recommendations from the Institute of Medicine call for 200 IU/d from birth through age 50 y, 400 IU for those aged 51–70 y, and 600 IU for those aged >70 y. Some experts say that optimal amounts are closer to 1000 IU daily. Until more is known, it is wise not to overdo it.” The only conclusion that the public can draw from this is to do nothing different from what they have done in the past.
The evidence in favor of higher 25(OH)D concentration and a higher RDA continued to grow in subsequent years. "Despite research on the association between low vitamin D status and many diseases, no consensus has emerged on the optimal serum 25(OH)D concentration. The concern is whether it is safe to maintain serum 25(OH)D concentrations in the range high enough to prevent some types of cancers and coronary heart disease," wrote Garland et al. 2014 in the American Journal of Public Health. In a meta-analysis of serum 25(OH)D and age-adjusted all-cause mortality, they showed that overall age-adjusted hazard ratios for mortality decline steeply with 25(OH)D for serum levels below 30 nmol/L, then gradually level off (Figure 3). The hazard ratio is not statistically different from 1 at 36 nmol/L.
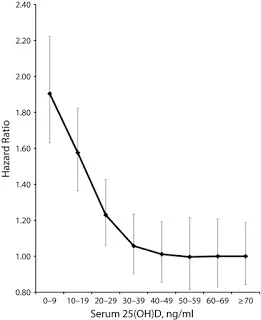
Figure 3. Source: Garland et al. 2014
In Finland, public health policy was changed in response to widespread low serum 25(OH)D concentration. Vitamin D fortification of certain dairy products and spreads began in 2002, and fortification levels were increased in 2010. This was successful in raising vitamin D intake, and health benefits are already measurable. In July 2017, Dimitrios Papadimitriou noted in the Journal of Preventive Medicine and Public Health the Type I diabetes, which had been on the rise, leveled off and then declined in Finland after the vitamin D fortification policy was implemented. Papadimitriou discusses vitamin D's role as a "powerful nuclear receptor-activating hormone of critical importance, especially to the immune system," and calls for public health authorities worldwide to modify RDAs in line with now quite substantive scientific research.
Papadimitriou titled his article "The Big Vitamin D Mistake," referring in a narrow sense to the IOM's statistical error. But he really discusses a mistake in a broader sense-- mounting evidence has been too slow to be incorporated into policymaking and practice.
Don't miss these other posts on diet and health and on fighting obesity:
- Stop Counting Calories; It's the Clock that Counts
- Forget Calorie Counting; It's the Insulin Index, Stupid
- Obesity Is Always and Everywhere an Insulin Phenomenon
- The Case Against Sugar: Stephan Guyenet vs. Gary Taubes
- The Case Against the Case Against Sugar: Seth Yoder vs. Gary Taubes
- How Sugar Makes People Hangry
- The Keto Food Pyramid
- Why a Low-Insulin-Index Diet Isn't Exactly a 'Lowcarb' Diet
- Hints for Healthy Eating from the Nurse's Health Study
- A Conversation with David Brazel on Obesity Research
- Mass In/Mass Out: A Satire of Calories In/Calories Out
- Carola Binder: The Obesity Code and Economists as General Practitioners
- Jason Fung: Dietary Fat is Innocent of the Charges Leveled Against It
- Faye Flam: The Taboo on Dietary Fat is Grounded More in Puritanism than Science
- Diseases of Civilization
- Sugar as a Slow Poison
- Katherine Ellen Foley—Candy Bar Lows: Scientists Just Found Another Worrying Link Between Sugar and Depression
- Ken Rogoff Against Sugar and Processed Food
- Kearns, Schmidt and Glantz—Sugar Industry and Coronary Heart Disease Research: A Historical Analysis of Internal Industry Documents
- Intense Dark Chocolate: A Review
- Salt Is Not the Nutritional Evil It Is Made Out to Be
- Whole Milk Is Healthy; Skim Milk Less So
- How the Calories In/Calories Out Theory Obscures the Endogeneity of Calories In and Out to Subjective Hunger and Energy
- Putting the Perspective from Jason Fung's "The Obesity Code" into Practice
- Julia Belluz and Javier Zarracina: Why You'll Be Disappointed If You Are Exercising to Lose Weight, Explained with 60+ Studies (my retitling of the article this links to)
- Meat Is Amazingly Nutritious—But Is It Amazingly Nutritious for Cancer Cells, Too?
- Diana Kimball: Listening Creates Possibilities
- On Fighting Obesity
- The Heavy Non-Health Consequences of Heaviness
- Analogies Between Economic Models and the Biology of Obesity
- Debating 'Forget Calorie Counting; It's the Insulin Index, Stupid'
Also see the last section of "Five Books That Have Changed My Life."
Relative Price Changes, 1997-2017

Hat tip to Shawn Ruest for flagging this article.
My inaugural lecture here at the University of Colorado Boulder, "Restoring American Growth," meditates on the issues raised by this graph.