Exorcising the Devil in the Milk

In honor of Halloween tomorrow, I will give sugar a holiday from my attacks. Today, the story is about an unhealthy aspect of milk that is actually avoidable without giving up dairy.
In brief, a mutation in cows about 8000 years ago switched amino acids and created a structural weakness at a key place in the important milk protein beta casein. This weak bond then allows 7-amino-acid “peptide” or fragment called BCM7 to break off. (See the image immediately below.) If this 7-amino-acid peptide “BCM7” gets through the intestinal wall it then wreaks havoc on health. And many, many people have “leaky guts” that allow these fragments to get through the intestinal wall.

Fortunately, there is still a substantial percentage of cows that have the original gene and produce milk without this problem. If cows are tested for which variant of the gene they have, then it is straightforward to get milk with the safe “A2” beta casein protein instead of milk with the unhealthy “A1” beta casein protein. And if bulls used for commercial breeding are tested for which of these genes they have, it is straightforward to switch over a herd from a mix of A1 and A2 cattle to a herd that produces only the safe A2 milk.
A2 milk may still have some of the health issues that have been identified for milk, but since most commercial milk in high latitudes is from herds with a lot of A1 genes, most of the evidence for problems from milk is from experiments using A1 milk. So the bottom line here is this answer to my question in another post, “Is Milk OK?”: A1 milk is definitely not OK; A2 milk may well be OK other than a general caution not to consume too much animal protein. (See “Meat Is Amazingly Nutritious—But Is It Amazingly Nutritious for Cancer Cells, Too?”)
In the Boulder area, A2 milk is available not only at Whole Foods but at Safeway. Because a key test is still under patent, certifiably A2 milk that is safe is only sold by the “a2 Milk Company.” Remember to buy only whole milk: I have a post “Whole Milk Is Healthy; Skim Milk Less So,” whose title is too positive if referring to A1 milk, but is about right when referring to A2 milk.
As it stands, the a2 Milk Company is dramatically understating the likely health benefits in its marketing. It is true that double-blind tests have not been done. The rest of this post details other types of evidence out there. In this, I draw on the book at the top, The Devil in the Milk: Illness, Health and the Politics of A1 and A2 Milk, by Keith Woodford. I will only present the basic case; the book itself does a great job of rebutting counterarguments. All of the quotations and graphs below are from this book.
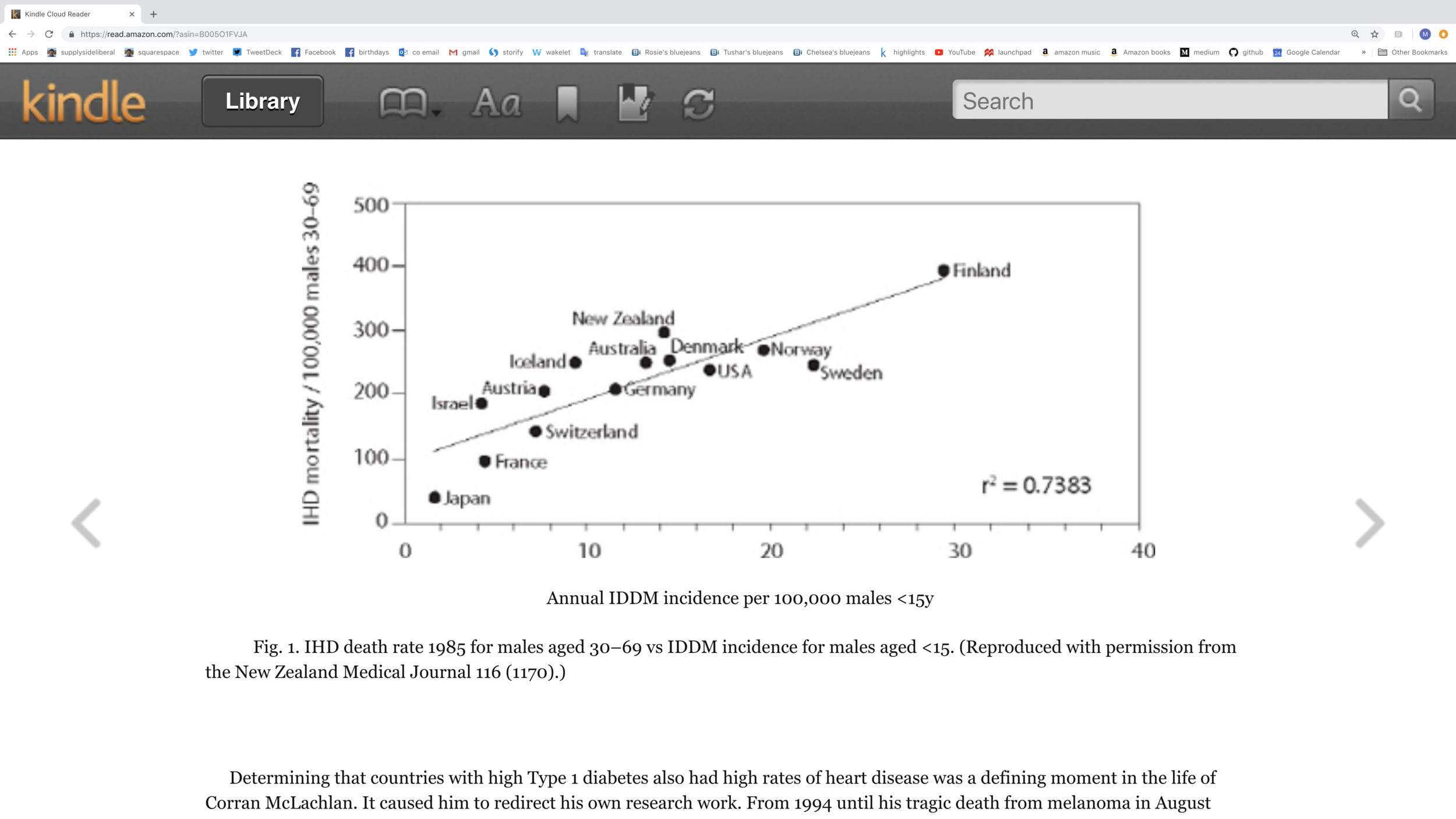
Before looking at direct evidence about A2 versus A1 milk, let me start with an intriguing fact: Type 1 diabetes (the autoimmune disease in which the body turns against and destroys its own insulin-producing cells) in children is very highly correlated across countries with heart disease in adults. (See the scatterplot in the screen shot just below.) Because heart disease is so much more common than Type 1 diabetes, this higher level of heart disease is too much to be caused by the higher levels of Type 1 diabetes. Both must have a third cause. (See “Cousin Causality.”) The set of countries is chosen as those that have good data on both diseases and are in a similar income range (so that poverty vs. riches is not a confounding factor).
Heart Disease: Below is the direct correlation between heart disease and A1 beta casein consumption across countries:

Here are some key passages about heart disease:
… the correlation between total dairy protein consumption and the incidence of male deaths from cardiovascular disease was quite weak, with an r2 of 0.26. When he looked at the relationship between the deaths and A2 beta-casein consumption it was even weaker, with an r2 of 0.16. However, the correlation between coronary heart disease and A1 beta-casein consumption was exceptionally high, at 0.71. When McLachlan excluded the A1 beta-casein from cheese consumption, the r2 value increased even further to 0.86 for male death rates in 1985 and 0.84 for the death rates in 1990. The justification for excluding cheese consumption from the analysis was based on theoretical (but not proven) evidence that the release of BCM7 is much lower from cheese than fresh milk. (Aspects of this were discussed in Chapter 2.) Female death rates followed a similar pattern, though with slightly lower r2 values.
The statistical tests show that the probability of getting chance or fluke results such as this, whereby the incidence of cardiovascular deaths can be explained to this extent by intake of A1 beta-casein, is less than one in a thousand for both males and females. …
McLachlan also compared the incidence of heart disease in the various states of West Germany. He found that 66% of the variation in deaths from heart disease could be explained by differences in the level of A1 beta-casein intake, based on the different breeds of cattle found in each state. Because there are only eight states, the correlation required for statistical significance was higher than for the other analyses. However, these results are significant at the 2% level (p< 0.02). This means that the likelihood of getting such a result by chance is less than one in fifty. …
Iceland and Finland provide some more interesting evidence. Ethnically, these Scandinavian peoples are very similar and they have similar diets. However, Finland has one of the highest levels of heart disease in the world, whereas in Iceland the incidence is only about 60% that of Finland. Is it coincidence that the intake of A1 beta-casein in Iceland is also only 60% that of Finland? (This difference in A1 beta-casein intake is because the Norske cows in Iceland have a higher level of A2 beta-casein and a lower level of A1 beta-casein in their milk than the Finnish cows.)
There are two other bits of evidence about heart disease. First, in rabbits prepared to be especially vulnerable to damaged arteries, A1 milk did much more artery damage than A2 milk. Second, it used to be a common recommendation that ulcer sufferers drink milk to reduce their symptoms. Doctors went away from this advice because it was found that drinking milk led to much higher rates of heart disease in ulcer sufferers. Note that ulcers are one type of “leaky gut.”
Type 1 Diabetes (the autoimmune disease): Below are scatterplots for Type 1 diabetes against A1 beta casein intake across countries on the left and for all beta casein intake on the right. Note how the relationship is tighter for A1 beta casein than for all beta casein. The r2 is 84% for A1 beta casein, only 46% for all beta casein (of which A1 beta casein is a part).

In addition to this cross-country evidence, there was a big, messed-up study of mice and rats in which the few non-messed-up comparisons possible show A1 beta casein causing Type 1 diabetes in two strains of rodents and no effect in one other strain.
Here is a key summary passage about Type 1 Diabetes that includes some additional bits of evidence:
All of the known jigsaw puzzle pieces linking A1 beta-casein and BCM7 to Type 1 diabetes have now been presented. Readers now need to make up their own minds as to whether the overall story is convincing. A brief summary of what we know and don’t know may help. We know for sure that there is a much higher rate of Type 1 diabetes in countries where there is a high intake of A1 beta-casein.
We know that statistically this is extremely unlikely to be due to a chance event. We also know that if A1 beta-casein is not indeed causative, no-one has been able to produce statistically significant evidence of the actual cause. What we cannot say is that we have 100% proof: we can only talk in terms of very high probabilities.
Animal trials seem to broadly confirm that A1 beta-casein can lead to diabetes. Bob Elliott found that casein diets were diabetogenic in BB rats back in the early 1980s, without knowing which particular component was the cause. Elliott and colleagues then found a very strong relationship between A1 beta-casein and diabetes in their colony of NOD mice. They also found that administration of naloxone, which counteracts the narcotic properties of opioids, stopped diabetes from developing in mice fed A1 beta-casein. Then the FAD trial showed that diabetes-prone BB rats in Canada had a higher rate of diabetes when fed A1 beta-casein in combination with Prosobee than when fed A2 beta-casein in combination with Prosobee, and that this difference was statistically significant. The rest of the FAD trial was a total mess.
Human blood tests indicate that Type 1 diabetics have more antibodies to A1 beta-casein than do non-diabetics, and these results are statistically significant. We also know that the only difference between A1 and A2 beta-casein is one amino acid in a string of 209, but that this single difference is what causes BCM7 to be formed during the digestion of A1 beta-casein. We also know that the BCM7 molecule formed from A1 beta-casein has a structure very similar to an amino acid sequence in the insulin-producing cells, and this provides a possible explanation of how antibodies attacking the BCM7 could also get confused and attack the insulin-producing cells. And we know that cattle infused with BCM7 have a reduced insulin response.
Autism and Schizophrenia: Here is a summary passage on autism and schizophrenia in relation to A1 and A2 milk:
It is now time to summarise the big picture in relation to autism and schizophrenia. It is apparent that many autistics and schizophrenics excrete abnormally high levels of BCM7 and other similar peptides in their urine. This declines markedly when these people are placed on a gluten-free and casein-free diet. The investigations by teams led by Cade, Reichelt and Shattock in three different countries confirm this.
We also know that BCM7 is released by the digestion of A1 beta-casein, but is either not released at all, or only in tiny amounts, from A2 beta-casein.
Numerous investigations show that eliminating casein and gluten from the diet leads to a marked improvement in the symptoms of autism. Once again Cade, Reichelt and Shattock stand to the fore, together with Reichelt’s colleague Ann-Mari Knivsberg. However, none of these medium- to long-term trials has been undertaken using double-blind protocols. Such trials are exceptionally difficult to conduct, but several are being planned. There is one published trial with significant results where the investigators were blind, and several other trials where they were not.
We also know that when BCM7 is injected into rats it causes them to act in a bizarre fashion, with many symptoms that resemble autism. Also, that the BCM7 enters many areas of the brain that are linked to autism, whereas similar peptides from gluten cannot access most of these areas.
We know that many thousands of parents of autistic children use a GFCF diet and believe it has benefits, but we also know that individual case studies such as this are not necessarily reliable.
We also have unsolicited testimonials supplied to A2 Corporation by parents of autistic children who have been given A2 milk. These parents believe their children are better on A2 milk than ordinary milk.12 Once again, these are only observational case histories that lack controls. However, these results seem plausible, in that we know there is unlikely to be a release of BCM7 from A2 milk.
Other Autoimmune Diseases and Allergies: For other autoimmune diseases, much of the evidence is about milk or beta casein in general. But BCM7 has the right kind of biological activity to be a prime suspect. For allergies and milk intolerance, anecdotal evidence is decent that A2 milk is less problematic. (Indeed, some people who think they are lactose intolerant might find they do OK with A2 milk.)
Once again, readers can now use the evidence to draw their own conclusions. In the case of milk intolerance and allergy, it seems likely that A1 beta-casein, and the milk devil BCM7 that is derived from it, are indeed implicated. Is it likely that so many consumers could all be wrong, particularly when the symptoms, such as diarrhoea, are well defined? Also, the story is totally consistent with what we know of the pharmacology and biochemistry of BCM7.
In the case of the auto-immune diseases discussed in this chapter, the story is somewhat more murky and speculative. What we do know for sure is that for each disease there is one or more environmental trigger. We also know that milk keeps coming up as a prime candidate. If milk contains the cause then it almost certainly has to be one or more bio-active proteins in the milk. It is also likely that opioids are involved. It is hard to go past BCM7 as a likely candidate.
Conclusion: As I mentioned above, this is only the basic case against A1 milk. Keith Woodford’s rebuttals of counterarguments are also very important. If you doubt the basic case, get the book on Kindle and check out the rest of the argument. To the simple counterargument “Why haven’t I heard this already?” there is a story of commercial and scientific politics, plus the simple fact that people can cook up arguments to disregard anything but expensive double-blind trials, and then argue that those arguments mean it isn’t worth doing those expensive double-blind trials.
Some New Zealand dairy farmers have been changing their herds over to A2 cows, but it is still a small fraction of all diary farmers there. If only a dairy powerhouse of New Zealand shifted to A2 herds more fully, it would change the commercial and scientific politics there, which in turn would help us get additional evidence about A1 vs. A2 milk.
In finding A2 dairy products, one basic fact to know is that the mutation at issue is mainly only in cows. Any goat dairy product is A2 and so safe in this sense. Buffalo dairy products (like the Buffalo mozzarella at Costco) is also A2. And the A1 gene is rare in sheep, which combined with the fact that BCM7 is probably not released as easily from cheese makes me feel safe with Manchego cheese from Costco, which is from sheep milk. Butter doesn’t have a lot of protein in it anyway, but I have been eating mostly goat milk butter from Whole Foods. Ghee, or clarified butter, is safe because it has no protein in it.
At retail, the thing I can’t yet find is A2 cream or A2 half-and-half. I have resorted to combining A2 milk with organic cream from Costco—which has some A1 protein in it, but hopefully not too much, since it is heavily fat.
Let me end by saying that the one thing I would be very scared to do would be to feed infants or young children regular A1 milk or the many dairy products (including many types of infant formula) that have A1 beta casein in them. Infants’ guts tend to be especially permeable to peptides like BCM7. Human milk is safe.
Someone asked me whether nursing mothers should avoid drinking A1 milk themselves. The answer to that is easy: nursing mothers should avoid A1 milk for the sake of their own health just like all other adults and children.
I. The Basics
II. Sugar as a Slow Poison
Best Health Guide: 10 Surprising Changes When You Quit Sugar
Heidi Turner, Michael Schwartz and Kristen Domonell on How Bad Sugar Is
Michael Lowe and Heidi Mitchell: Is Getting ‘Hangry’ Actually a Thing?
III. Anti-Cancer Eating
How Fasting Can Starve Cancer Cells, While Leaving Normal Cells Unharmed
Meat Is Amazingly Nutritious—But Is It Amazingly Nutritious for Cancer Cells, Too?
IV. Eating Tips
Using the Glycemic Index as a Supplement to the Insulin Index
Putting the Perspective from Jason Fung's "The Obesity Code" into Practice
Which Nonsugar Sweeteners are OK? An Insulin-Index Perspective
V. Calories In/Calories Out
VI. Wonkish
Anthony Komaroff: The Microbiome and Risk for Obesity and Diabetes
Carola Binder: The Obesity Code and Economists as General Practitioners
Analogies Between Economic Models and the Biology of Obesity
VIII. Debates about Particular Foods and about Exercise
Jason Fung: Dietary Fat is Innocent of the Charges Leveled Against It
Faye Flam: The Taboo on Dietary Fat is Grounded More in Puritanism than Science
Confirmation Bias in the Interpretation of New Evidence on Salt
Julia Belluz and Javier Zarracina: Why You'll Be Disappointed If You Are Exercising to Lose Weight, Explained with 60+ Studies (my retitling of the article this links to)
IX. Gary Taubes
X. Twitter Discussions
Putting the Perspective from Jason Fung's "The Obesity Code" into Practice
'Forget Calorie Counting. It's the Insulin Index, Stupid' in a Few Tweets
Debating 'Forget Calorie Counting; It's the Insulin Index, Stupid'
Analogies Between Economic Models and the Biology of Obesity
XI. On My Interest in Diet and Health
See the last section of "Five Books That Have Changed My Life" and the podcast "Miles Kimball Explains to Tracy Alloway and Joe Weisenthal Why Losing Weight Is Like Defeating Inflation." If you want to know how I got interested in diet and health and fighting obesity and a little more about my own experience with weight gain and weight loss, see “Diana Kimball: Listening Creates Possibilities” and my post "A Barycentric Autobiography.