Less Than 6 or More than 9 Hours of Sleep Signals a Higher Risk of Heart Attacks

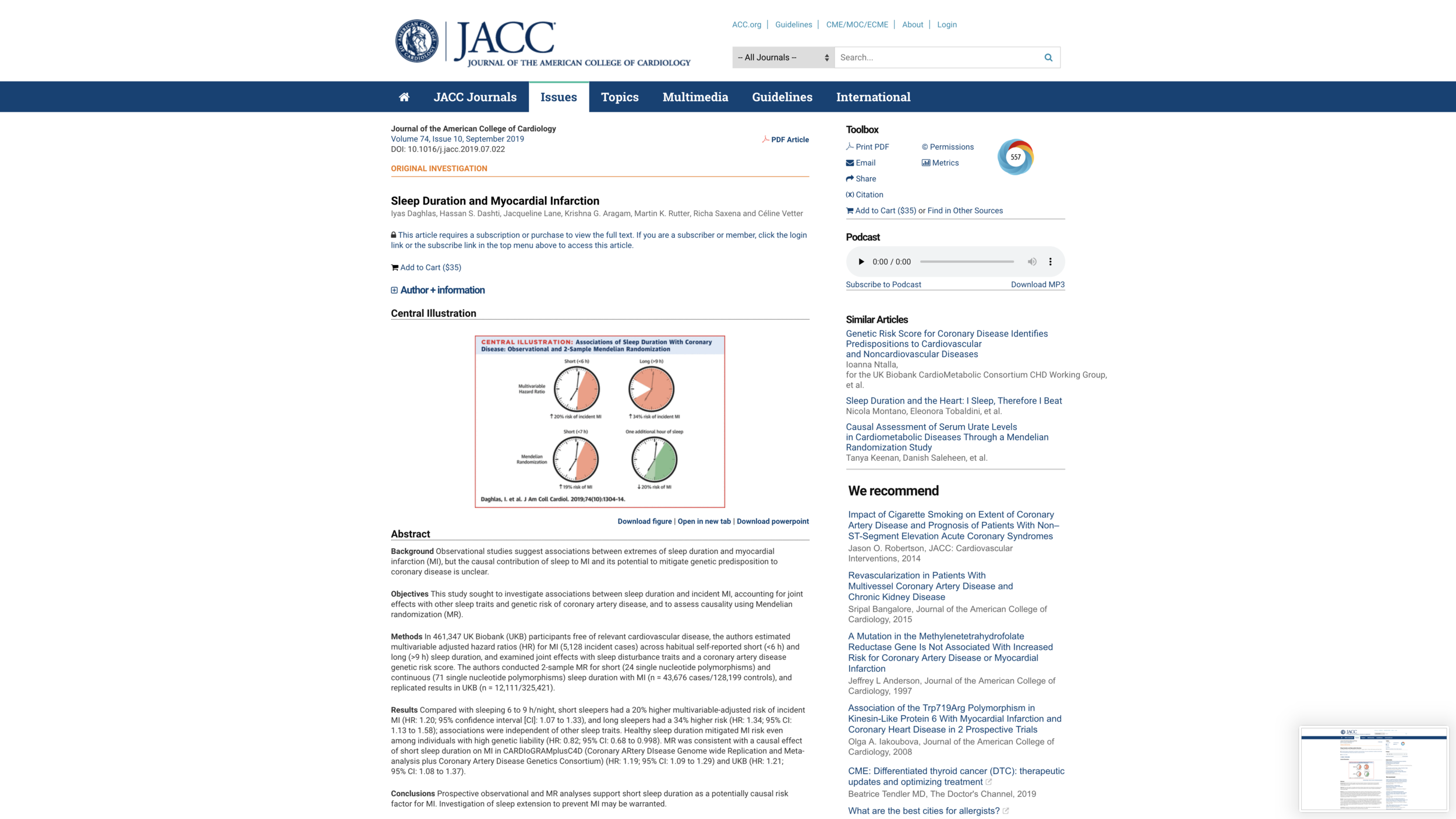
It is a good thing that our culture’s attitudes toward sleep are turning more positive—from thinking of sleep as a sign of lazy slothfulness to thinking of sleep as an important contributor to creativity and good health. The authors of the Journal of the American College of Cardiology paper “Sleep Duration and Myocardial Infarction,” have made an important contribution to this ongoing cultural shift: Iyas Daghlas, Hassan S. Dashti, Jacqueline Lane, Krishna G. Aragam, Martin K. Rutter, Richa Saxena, and Céline Vette. The strength of the signal of heart attack risk provided by habitually short or habitually long sleep is substantial, as the paper’s “Central Illustration” shown above reports: when reporting an integer number of hours, integers 5 or below predict 1.2 times as high a risk as integers 6-9, while integers 10 and above predict 1.34 times as a high a risk as integers 6-9.
Because habitually short or long sleep reported at a baseline interview predicted later heart attacks, it is clear that those with unusually short or long sleep should take extra efforts to reduce heart attack risk. The authors of “Sleep Duration and Myocardial Infarction” also go some part of the way toward suggesting that interventions to moderate habitually short sleep might help reduce heart attack risk. They are careful not to oversell this possibility, saying:
“… randomized trials of sleep extension will be the most rigorous test of causality.”
and
“… recent work has demonstrated that sleep extension for short sleepers is a feasible intervention.”
referencing:
Al Khatib HK, Hall WL, Creedon A, et al. Sleep extension is a feasible lifestyle intervention in free-living adults who are habitually short sleepers: a potential strategy for decreasing intake of free sugars? A randomized controlled pilot study. Am J Clin Nutr 2018; 107:43–53.
Mendelian Randomization
In “Sleep Duration and Myocardial Infarction,” the closest the authors get to causal evidence that interventions to moderate habitually short sleep might reduce heart attack risk is through their “Mendelian Randomization” analysis. Mendelian Randomization is a technique that treats genes as an instrument for traits the genes foster. I discussed one of the few truly convincing Mendelian Randomization studies in “Data on Asian Genes that Discourage Alcohol Consumption Explode the Myth that a Little Alcohol is Good for your Health.” The Mendelian Randomization evidence in “Sleep Duration and Myocardial Infarction” is more convincing than that in many Mendelian Randomization studies, but still far from fully convincing. Let me explain. The point estimate in need of interpretation is that an extra hour of sleep caused by genes for more sleep predicts heart attack .8 times as much, with a 95% confidence interval from .67 to .95. (In percentage reductions, an extra hour of sleep caused by genes for more sleep predicts a 20% lower risk of heart attacks relative to the base rate for heart attacks, with a 95% confidence interval from a 5% reduction to a 33% reduction relative to the base rate.)
The big interpretative issue can be stated succinctly this way: an intervention that gets people to sleep longer is not likely to have the same effects as hypothetical engineering that altered an individual’s genes at conception.
Another issue that will soon be resolved by data sets with having genetic data for the parents as well as the individuals themselves is that an individual’s genes represent half of the genes the individual’s two biological parents have, and those genes in the parents are likely to affect the kind of parenting they give in relation to sleep.
Typically, hypothetical genetic engineering will have a bigger effect because it works through many channels throughout life. Let me give a simple example from economics. There are no doubt genes that predispose people to take courses on financial planning. Indeed, I would bet that with a data set that had the genes of a 100 million people and detailed data on the courses they have taken, we would have no trouble finding those genes. But it would be a mistake to take those genes as good instruments for the effect of taking courses on financial planning on patterns of retirement saving. The reason is that genes for taking courses in financial planning are likely to be genes for intelligence—especially mathematical intelligence—and for interest in finance. Mathematical intelligence and being interested in finance would be likely to help people do a better job of retirement saving in many ways even if for some reason they never take a financial planning class.
The fact that the biggest, most important genes for cardiovascular risk are known, and that sleep duration is predicted by many genes that each are a small part of the story allows the authors of “Sleep Duration and Myocardial Infarction” to use a variety of techniques to reasonably rule out the possibility that causally distinct genes near on the chromosome—and thereby highly correlated with sleep duration genes—are confounding the inference that sleep duration genes cause more heart attacks. But the key issues of interpretation remain.
After correlated gene effects are ruled out, that genes for getting more sleep predict that someone will be more likely to get a heart attack says that either getting more sleep reduces heart attack risk, or something that causes people to get more sleep (intermediate in the causal chain between those genes and sleep duration itself) reduces heart attack risk or both. It is easy to think of many, many things that might both cause someone to get more sleep and to have reduced heart attack risk. For example, many things that operate through the cognitive and social realm could both cause someone to get more sleep and to have reduced heart attack risk: intelligence, education, the likelihood a relative is a doctor, the type of friends one has. And the biology of sleep has enough unknowns to leave room for many biological states that could both cause someone to get more sleep and to have higher heart attack risk.
The authors of “Sleep Duration and Myocardial Infarction” try to control for some of the most obvious things that might cause both more sleep and fewer heart attacks. But statistical controls are seldom adequate to do the necessary “controlling.” Even for the things they are intended to measure, available data is usually error-ridden—and careful measurement-error correction is uncommon. And a host of things that could be relevant (especially given the limited state of our knowledge) may not be measured at all.
Nevertheless, knowing that either or both getting more sleep reduces heart attack risk, or something that causes people to get more sleep (intermediate in the causal chain between those genes and sleep duration itself) reduces heart attack risk is extremely helpful. Even if an intervention trial showed no effect of directly getting people to sleep more on heart attack risk, the search for something that causes both more sleep and reduced heart attack risk could be a very fruitful one in medical insights.
Two related reminders may jump-start interpretation in other cases when Mendelian Randomization is used as a technique:
Genes for sleep causing reduced heart attack risk does not mean more sleep causes reduced heart attack risk. A third thing downstream from genes for sleep could cause both more sleep and reduced heart attack risk. (See “Cousin Causality.”) To generalize, genes for X causing Y does not mean X causes Y. The key alternative is that “genes for X” cause Z, and Z causes both X and Y.
A feasible intervention might be very different in its effects from what would happen if one could really do genetic engineering at conception (as well as genetic engineering at the conception of the parents).
The authors cite the following paper as saying Mendelian Randomization is not susceptible to reverse causality:
Davey Smith G, Ebrahim S. ‘Mendelian randomi- zation’: can genetic epidemiology contribute to un- derstanding environmental determinants of disease? Int J Epidemiol 2003;32:1–22.
This is simply not true in any useful sense. Supposed one is interested in whether X causes Y. Genes for X can easily be “genes for X” precisely because they cause Y, which then in turn causes X. What is most helpful here is the concept of “genetic correlation”: loosely, some of the “genes for X” also being “genes for Y.” Just as correlation does not imply causation, genetic correlation doesn’t imply causation. There is a danger that some scientists will be tempted (and fall for the temptation) to use the rhetoric of Mendelian Randomization to try to get causation from genetic correlation. Instead, one should think of getting an implication of causation from a genetic correlation as requiring additional arguments that are just as difficult as—and indeed are mostly analogous to—the arguments needed to get an implication of causation from any other type of correlation.
The Bottom Line
Despite all of the care that should be taken in interpreting the science, the results of “Sleep Duration and Myocardial Infarction” should certainly raise one’s Bayesian assessment to a substantial posterior that arranging your life so that you get nearer to 7 or 8 hours sleep will reduce your risk of a heart attack. For now, that is the bottom line you should take in terms of advice for your own life.
I should also mention that if more sleep does reduce heart attack risk, one important possibility channel is that lack of sleep leads people to eat worse by reducing their self-control. If so, then having a pattern of eating that doesn’t depend on so much self-control in order to eat well could help reduce the harm if one can’t find time to get enough sleep. (See “Live Your Life So You Don't Need Much Self-Control.”) And, of course, arranging your life so it doesn’t take so much self-control to get enough sleep can help if sleep reduces heart-attack risk through other channels.
For annotated links to other posts on diet and health, see: