Which Nonsugar Sweeteners are OK? An Insulin-Index Perspective
In my view, one of the greatest steps forward for public health would be for people to get the message that sugar is very bad—worse than many other foods that people worry about. (See “The Trouble with Most Psychological Approaches to Weight Loss: They Assume the Biology is Obvious, When It Isn't” and the posts listed below under the heading “Sugar as a Slow Poison.”)
Given the dangers of sugar, it is natural to ask whether any nonsugar sweeteners are OK. One part of the answer is that sweetness itself tends to make you think about food, and thinking about food can make you hungry. This is called the cephalic response. It is like the effect of walking past a restaurant. The cephalic response getting your body prepared for food is OK if you are just sitting down to eat anyway, but it could be a big problem if you are, say, drinking diet sodas between meals, since it will make you hungry when you weren’t otherwise going to eat.
Are there any nonsugar sweeteners that are OK other than the cephalic response of making you think about food and getting your body prepared for food? The excellent article flagged above, “The Skinny on Sweeteners” by Adam Nally, gives this answer, which accords with my own views:
I’ve been using ketogenic diets since 2005. In that time, I have found personally, and clinically with the patients in my practice, that combinations of Stevia, chicory root and erythritol, when used in baking, seem to provide adequate texture and remove any aftertaste that may be found when using them individually. These combinations also have no effect on weight loss, weight regain or adverse metabolic changes when used with a ketogenic lifestyle.
These sweeteners are equally OK when used in other ways than in baking.
Bad Sweeteners
Adam has a nice paragraph about insulin:
… weight gain and weight loss are controlled by 30 different known hormones, the master hormone being insulin, our overall goal is to lower the insulin levels in the blood stream. Glucose (a carbohydrate in its most simple form) stimulates insulin to rise. A Low carbohydrate diet works because insulin levels are significantly lowered throughout the day. Elevation in cholesterol, elevation in triglycerides and production of uric acid occur because of insulin surges. The presence of glucose (from carbohydrates or sugars) is the most common stimulus for insulin to rise.
This is in line with what I say in “Obesity Is Always and Everywhere an Insulin Phenomenon.”
The following forms of sugar all raise insulin levels:
… white and brown sugar, fructose, succanat, corn syrup, high fructose corn syrup, honey, malt syrup, cane juice, cane syrup, rice syrup, barley syrup, maple syrup, molasses, turbinado, agave, monk fruit and fruit juice concentrate.
Adam has this additional useful caution:
Beware of products that contain “no added sugar” because they will often contain sugar concentrates in the form of concentrated grape or apple juice.
Fructose is sometimes promoted as a suitable sweetener for patients with diabetes or people who are wanting to follow a low-carb diet; however even though it does not cause a significant insulin rise on its own, it is rapidly absorbed by the liver and converted into glycerol which leads to increased insulin level a few hours later, as well as raising triglyceride and cholesterol levels.
In addition, relying on the article above, experiments indicate that the following nonsugar sweeteners raise insulin levels:
acesulfame potassium (Ace-K™, Sunette™)
saccharine
maltitol
sorbitol
xylitol
sucralose crystallized by being bound to dextrose or maltodextrin, as it is in Splenda™— sucralose is only OK in its liquid form)
Adam is not entirely clear about lactitol and hydrolyzed starch hydrolysates (HSH), but reading between the lines, he seems to be saying they are not as bad as maltitol, sorbitol or xylitol, but he doesn’t recommend them.
Cyclamate is banned in the United States because it causes bladder cancer in rats; otherwise Adam describes it as similar to sucralose: any dextrose or maltodextrin it is combined with will raise insulin.
Aspartame does not seem to raise insulin, but has a different downside:
… because of recent evidence demonstrating the effect of aspartame on the gut bacteria, changes in brain mitochondria with prolonged exposure, and stress responses effecting gluconeogensis (glucose regulation) in the liver, [Adam Nally] recommends avoiding this sweetener or using it with great caution in the short term only.
If you think an effect on gut bacteria is no big deal, I hope you will think otherwise after reading my post “Anthony Komaroff: The Microbiome and Risk for Obesity and Diabetes.”
OK Sweeteners
Let me summarize by quoting short bits about the sweeteners that are OK—except for making you think about food because of their sweetness:
Fructooligosaccharides (FOS) … are actually short chain fibers derived from inulin. … They are commonly derived from chicory root, bananas, onions, garlic and the blue Agave. … A great option that Dr. Nally recommends for use in cooking is a combination of FOS with erythritol called Swerve.
Erythritol is absorbed and excreted unchanged and appears to have no insulin response (Food and Chemical Toxicology, Dec 1998, Volume 36, Issue 12, Pages 1139-1174).
The Dispute about Stevia
In general, Adam’s article is an excellent article on nonsugar sweeteners. But on Stevia, what Adam says is in direct contradiction with what Jason Fung says in The Obesity Code about Stevia (See “Obesity Is Always and Everywhere an Insulin Phenomenon.”) Here are the two quotations:
Adam Nally: Stevia in the liquid form is a non-caloric natural sweetener which contains no carbohydrate. It is derived from a South American shrub and has been widely available for use in Asia for many years.
… Stevia does not increase blood sugar and appears to improve insulin sensitivity in the pancreas (Metabolism, 2003 Mar;52(3):372-8.).
Jason Fung: The important question is this: Do artificial sweeteners increase insulin levels? Sucralose raises insulin by 20 percent, despite the fact that it contains no calories and no sugar. This insulin-raising effect has also been shown for other artificial sweeteners, including the “natural” sweetener stevia. Despite having a minimal effect on blood sugars, both aspartame and stevia raised insulin levels higher even than table sugar.
This dispute should be possible to resolve with additional lab experiments with human subjects. I’d be glad for any references that illuminate the situation for stevia.
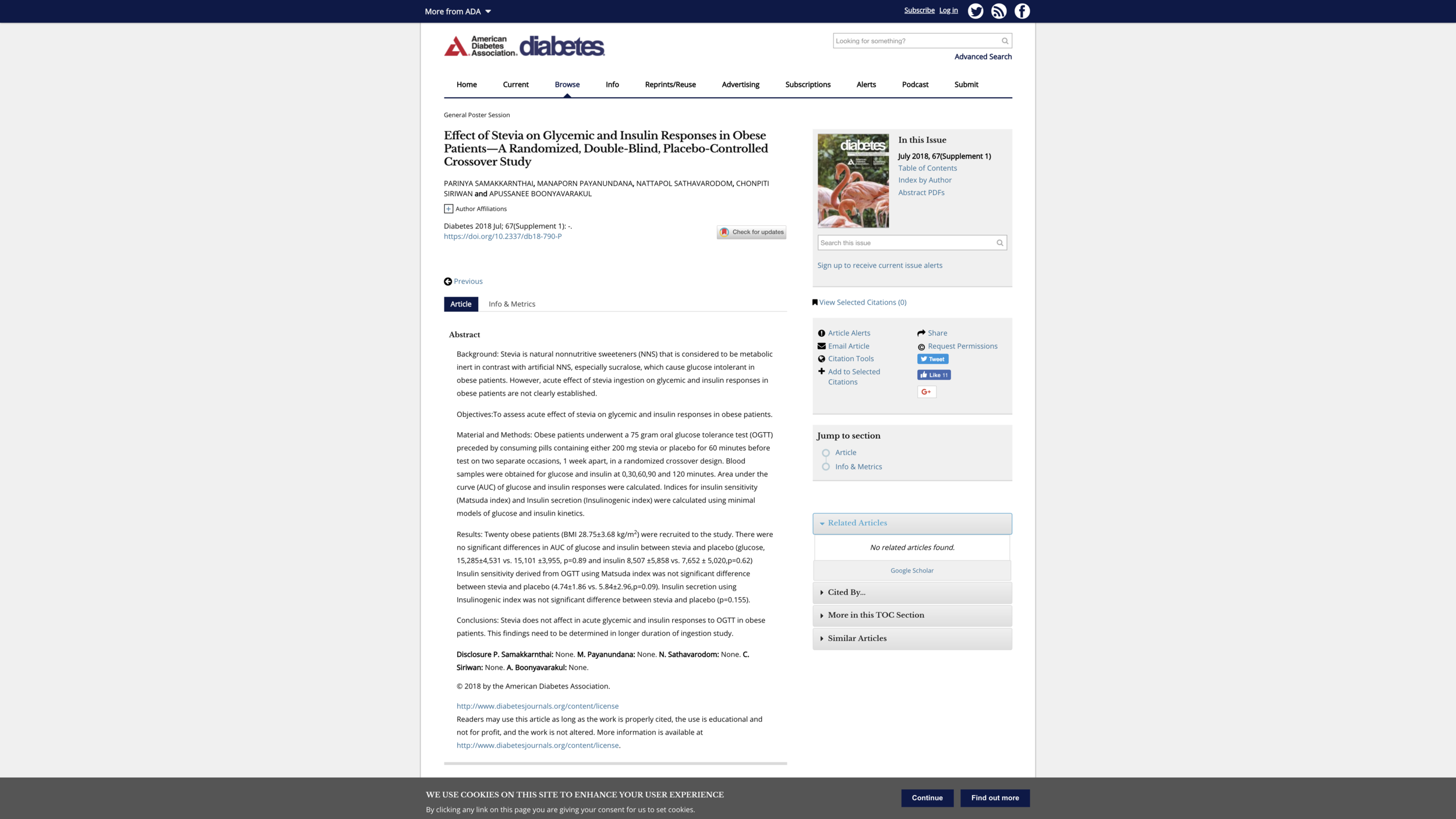
Stevia Update, January 19, 2019: In a study with what sounds like a good design, bringing 20 obese individuals in twice wasn’t enough to get great precision, but the effects of Stevia on insulin didn’t look that much different from the effects of a placebo. Here is the bottom line:
… between stevia and placebo (glucose, 15,285±4,531 vs. 15,101 ±3,955, p=0.89 and insulin 8,507 ±5,858 vs. 7,652 ± 5,020,p=0.62) Insulin sensitivity derived from OGTT using Matsuda index was not significant difference between stevia and placebo (4.74±1.86 vs. 5.84±2.96,p=0.09). Insulin secretion using Insulinogenic index was not significant difference between stevia and placebo (p=0.155).
Conclusions: Stevia does not affect in acute glycemic and insulin responses to OGTT in obese patients. This findings need to be determined in longer duration of ingestion study.
Note that this result was based on getting Stevia in a pill, so it doesn’t include the cephalic effect of sweetness itself. See below:
For annotated links to other posts on diet and health, see:
For example, here is what the first section looks like:
I. The Basics